
Research Article | DOI: https://doi.org/10.31579/2578-8868/192
1,2* Clermont Université, université d’Auvergne, Neuro-Dol, BP 10448, F-63000, Clermont-Ferrand & Inserm U1107, F-63001 Clermont-Ferrand, France
2 VITROBIO SAS & NATURVEDA SAS, laboratoire pharmaceutique
1 Clermont Université, université d’Auvergne, Neuro-Dol, BP 10448, F-63000, Clermont-Ferrand & Inserm U1107, F-63001 Clermont-Ferrand, France
*Corresponding Author: Rémi Shrivastava, Clermont Université, université d’Auvergne, Neuro-Dol, BP 10448, F-63000, Clermont-Ferrand & Inserm U1107, F-63001 Clermont-Ferrand, France
Citation: Rémi Shrivastava, Gisela DA Silva Borges, François Gabrielli, Ravi Shrivastava, Lénaïc Monconduit (2021) Mig-RL: a Natural Preventive Treatment Against Migraine. Outcomes of a Randomized, Double-Blind Clinical Trial. J. Neuroscience and Neurological Surgery. 9(2); DOI:10.31579/2578-8868/192
Copyright: © 2021 Rémi Shrivastava, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 15 June 2021 | Accepted: 29 June 2021 | Published: 05 July 2021
Keywords: migraine; tanacetum parthenium; salix alba
BACKGROUND
The efficacy and safety of Mig-RL (Commercial name HERBA MIG), a synergistic association of two plant extracts, Tanacetum parthenium (150mg, 0.5% parthenolide) and Salix Alba (150mg, 25% salicin) were investigated as a preventive treatment for episodic migraine. Mig-RL was compared with a placebo in a randomized, double-blind clinical trial.
MATERIALS AND METHODS
This trial included 129 patients having episodic migraine and diagnosed with migraines without aura for over a year and meeting the migraine criteria, as defined in the International Classification of Headache Disorder (ICHD-3 :1.1). P). Baseline data was collected for 28 days before the start of the three-months treatment period. Patients were randomized in a 1:1 ratio to receive either Mig-RL (a single dose of 300mg per day, per os) or placebo (identical capsules containing 300 mg starch, 1 per day, per os) for a period of 12 consecutive weeks. The primary endpoint was the mean change in the average number of migraine days per month, comparing the baseline 28-days pre-intervention period with the weeks 9 to 12 after the first dose of the trial regimen. Secondary endpoints were the percentage of patients with a reduction of at least 30% in the average number of migraine days per month and days of use of any acute headache medication per month. The HIT-6 and MIDAS scores were also evaluated vs. baseline between the two groups.
RESULTS
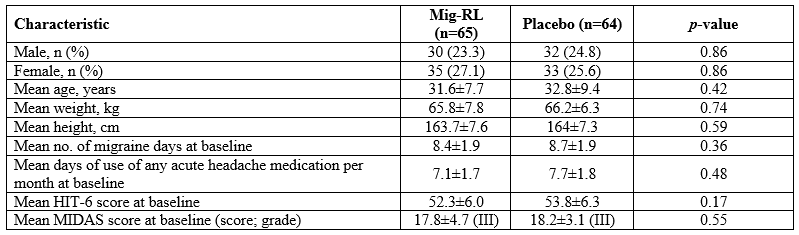
Out of 172 patients enrolled, 129 were randomly assigned to the Mig-RL arm (n=65) or the placebo arm (n=64). The mean (±SD) number of baseline migraine days per month was 8.4±1.9 and 8.7±1.9, respectively. The mean reduction in the average number of migraine days per month was 2.5±0.4 (p<0.001) with Mig-RL and 1.9±0.4 (p<0.001) with placebo. A difference of 0.6±0.4 (p=0.01) between the two groups.
The percentage of patients with at least 30% reduction in average number of migraine days per month was 49% in Mig-RL and 32% in placebo (p<0.05 vs. placebo). Only a few isolated and minor side effects were reported and overall Mig-RL was well tolerated by patients.
CONCLUSIONS
Mig-RL, a synergistic combination of two plant extracts, seems to have a moderate effect in the prevention of migraines. Without side effects, the combination of Tanacetum parthenium and Salix alba could be an additional help for some patients. However, further investigations and an improvement in the quality of the plants are still necessary.
Migraine is a chronic neurological disease characterized by the presence of several incapacitating neurological symptoms, such as headaches, sensitivity to light and sound, and nausea. Migraine can be episodic or chronic, based on the number of headaches days per month [1]. Episodic migraine is described as migraine with or without aura occurring in a headache pattern of <14 days per month [2]. Migraine without aura manifests in attacks lasting 4 to 72 hours; the headaches are characterized by their unilateral location, pulsating quality, moderate or severe intensity, aggravated by routine physical activity and associated with nausea and/or photophobia and phonophobia [1]. Migraine with aura is primarily characterized by the focal neurological symptoms that usually precede the headache. Chronic migraine, on the other hand, refers to patients manifesting long-duration headaches (≥15 days / month) [3].
Migraine affects over 1 billion individuals worldwide, making migraine the third leading cause of disability worldwide [4] Migraine symptoms interfere with normal day-to-day life, including family, education, work, and contributing to the development of comorbidities such as cardiovascular disease, depression and anxiety [5]
Migraine management is based either on non-pharmacological approaches, such as suppressing triggering factors (if they are known), or pharmacological approaches, such as abortive (acute) treatment and/or preventive (prophylactic) treatment [6]. The recommendations for using pharmacological migraine prevention vary greatly between published treatments guidelines. As a general rule, migraine prevention should be considered when attacks affect quality of life and is indicated in roughly one third of migraine patients [6], [7]. The comorbidities should be taken into account when considering and selecting an approach to prevent migraine attacks.
The following classes of medications are used for migraine prevention: antiepileptic drugs, antidepressants, beta blockers, injectable calcitonin gene-related peptide (CGRP) monoclonal antibodies, calcium channel antagonists, serotonin antagonists, botulinum neurotoxins, NSAIDs, and others including cyanocobalamin, riboflavin, tryptophan and magnesium [6]. A drug is chosen based on its efficacy, its safety profile, the patient’s preference, and the presence of any coexistent or comorbid conditions. All these therapies are symptomatic, often have insufficient efficacy, and may have variable side effects [8]. Part of current research is now targeting herbal products to treat migraine patients (adults and children) [9]. Because herbs, spices, and their active constituents can influence many processes associated with migraine pathophysiology, they can be used as an alternative or adjunct intervention to enhance current treatment outcomes [10]. Moreover, their natural aspects make them more accepted by the patients, as they usually induce fewer side effects compared to traditional chemical drugs.
Tanacetum parthenium L. belongs to the Asteraceae family and is a perennial herb commonly known as Feverfew. Tanacetum parthenium contains many sesquiterpene lactones, where the most abundant is the parthenolide (up to 85% of the total sesquiterpene content), in the leaves and the flower heads [11]. However, flower heads and leaves differ in quali-quantitative component profile (e.g. parthenolide is higher in the flower heads than in the leaves) [12]. The plant also contains a high percentage of sterols and triterpenes in the roots [13]. Its medical properties against inflammation and vertigo have been known for a long time and Tanacetum parthenium is traditionally used as an antipyretic and for the treatment of arthritis, headaches, insect bites, spasms, and menstrual disorders [13]. More recently, Tanacetum parthenium has been extensively studied for migraine treatment and prophylaxis. The results obtained so far corroborate its efficacy [14]. Antinociceptive, anti-inflammatory and anti-serotonin features were preclinically described [15]–[17]. As mentioned above, therapeutic effects are generally attributed to leaves and/or flowers. This is mainly due to the presence of sesquiterpene lactones and flavonoids, which are also found in abundance in the plant[13]. The lipophilic character of parthenolide seems to enhance particularly well the passage through the blood brain barrier [18]. Tanacetum parthenium also shows a good safety profile) [19].
In the past, Shrivastava et al. have shown, in a prospective pilot open-label study, the prophylactic efficacy of a combination of Tanacetum parthenium (150mg) and Salix alba (150mg) when administered twice a day (Mig-RL®) [20] The latter is traditionally recognized for its analgaesic effects, mainly due to the presence of salicin, precursor of salicylic acid (aspirin). To confirm these results with a more robust methodology and to study the efficacy of a slightly optimized formula of Mig-RL®, we conducted a 16-weeks, double-blind, randomized, placebo-controlled clinical study to evaluate the efficacy, safety and side effects of the association of Tanacetum parthenium (150 mg with at least 0.5% of parthenolide) and Salix alba (150 mg with at least 25% of salicin) plant extracts, administered once a day (Mig-RL®, VITROBIO-NATURVEDA, France) [20].
Trial oversight
The protocol was approved by relevant ethics committees (Ashirwad Ethics Committee) and institutional review boards. While conducting the study, the authors vouch for the adherence to the protocol, the accuracy and completeness of data and analyses, and the report of adverse events. The trial complied with the International Conference on Harmonisation Guidelines for Good Clinical Practice, the principles of the Declaration of Helsinki, relevant national and local regulations. At the time of screening, participants signed consent forms. The trial sponsor, VITROBIO NATURVEDA SAS, provided the trial medication and performed the data analysis. An independent organization Pharmazone (CIN:U51397AS2014PTC011790) was commissioned to audit and validate the proper respect of the processes established by the protocol throughout the duration of the study. After validation, Pharmazone was responsible for forwarding the anonymised results to the sponsor.
Trial Participants

This double-blind, randomized, placebo-controlled study was performed at the Mudra ClinCare Hospital in Mumbai, India. The first patient was recruited in June 2017 and the last patient monitored was in May 2019. The patients eligible to enter this study were aged between 18 and 55 years old, males or females [21]. All patients had been diagnosed for over a year with migraines without aura and met the definition of the International Classification of Headache Disorder version 3 [2]. 28 days of observation before the start of the three-months treatment period was used to establish the baseline. To maintain group homogeneity, patients with less than five days of migraine a month or migraine attacks lasting less than four hours were not included in the study. Participants were asked to keep a migraine diary for more than six months to evaluate the frequency of migraines and medication use. Patients that had been using a new treatment for their attacks less than six months prior to the study were not retained, nor were patients who were diagnosed headaches induced by medication overuse. Crisis treatments were authorized to the patients during the study period only if they had been using it for more than six months. All treatments with aspirin, salicylates or herbal extracts were prohibited during the study.
The main non-inclusion criteria were allergies to salicylates and camphor or hypersensitivity to study medication, drug abuse or dependency, chronic psychiatric or systemic diseases, pregnant women, breastfeeding women. Subjects taking antidepressants, neuroleptics, anxiolytics or prophylactic treatment for migraine within three months before the start of the study, were also excluded. The exclusion criteria were chosen for a safety matter and to avoid bias of the final results.
Trial End Points
The primary end point was the mean change in the average number of migraine days per month, comparing the baseline 28-day pre-intervention period with the weeks 9-12 after the first dose of the trial regimen [22].
Secondary end points were to compare the average number of migraine days per month, in between the baseline 28-day pre-intervention period and the weeks 1-4 and 5-8 after the first dose of the trial regimen.
Secondary end point were also to determine the percentage of patients experiencing a reduction from at least 30% to 50% on their average migraine days per month, and the mean change in between the baseline on the average number of days per month in which acute migraine medication was used and the weeks 9 to 12.
A migraine day was defined as any day on which the patient had a migraine or probable migraine. Defined in a calendar day, in which headache pain lasted, at least, 4 consecutive hours and met criteria for migraine or probable migraine (subtype in which only one migraine criterion is absent), or a calendar day in which acute migraine–specific medication was used to treat a headache of any duration [22].
Other secondary end points included the mean change in the score on the six-item Headache Impact Test (HIT-6) and the Migraine Disability Assessment (MIDAS).
HIT-6 and MIDAS tests were designed to provide a global measure of adverse headache impact. HIT-6: scores range from 36 to 78, with higher scores indicating a greater degree of headache-related disability. MIDAS scores are interpreted as grade I = 0–5 (minimal or infrequent disability), grade II = 6–10 (mild or infrequent disability), grade III = 11–20 (moderate disability), grade IVa = 21–40 and higher (severe disability), grade IVb = 41 and higher (very severe disability) with higher scores indicating greater disability and decreased scores consistent with improvement [23], [24].
Safety and side-effect profiles were evaluated according to reported adverse events, vital signs (systolic and diastolic blood pressure, pulse, body temperature, and respiratory rate), physical examination, cardiovascular, respiratory system, gastrointestinal system, musculoskeletal and nervous system examination.
Study design
This randomized, double-blind, placebo-controlled trial consisted of a screening visit, a 28-day pre-intervention period, and a 12-week intervention period, with a final evaluation in week 12 [22]. Based on the screening visit and information collected in a daily diary during the pre-intervention period, patients were enrolled or excluded from the trial.
Patients satisfying all the ICHD-3 inclusion criterias and none of the exclusion criterias were enrolled and randomly allocated to a 1:1 ratio as per randomization schedule to receive Mig-RL or placebo. Randomization was performed by using SAS Version 9.1.3. The randomization schedule was generated with block randomization methodology.
Patients were seen at five scheduled visits for protocol-specified evaluations: at screening, baseline, week 4, week 8, and week 12, or at the time of early withdrawal from the trial. Patients who withdrew prematurely had final protocol-specified evaluations performed as soon as possible after withdrawal. Headache data (e.g., occurrence, duration, and pain severity; occurrence of photophobia, phonophobia, nausea, or vomiting; and any use of migraine medication) were captured daily through an individual headache diary.
Treatment
As per the randomization, patients received either Mig-RL or the placebo. Mig-RL treatment group received capsules containing standardized powdered extract of Tanacetum parthenium 150 mg and Salix alba 150 mg, characterized by chromatography according to the European Pharmacopoeia, with clear instructions of use (one capsule / day; per os). The extracts contained in the capsules were supplied by the laboratory VITROBIO-NATURVEDA according to their extraction process: water/ethanol (70/30) for a ratio plant extract 3-4/1. The parthenolide content of Tanacetum parthenium was at least 0.5% and the salicin content in Salix alba was at least 25%. Both plant extracts are listed in the European Pharmacopoeia and are authorized for oral administration to human beings by the European Union Regulatory Authorities. Placebo patients received starch containing capsules (300mg), with the same instruction as the treatment group (one capsule / day: per os).
Statistical analysis
Estimations based on the observational trial of Mig-RL in episodic migraine [20] and the Cochrane systemic review to evaluate the efficacy of Tanacetum parthenium as a preventive treatment for migraine [14] predicted that a sample of 80 patients who had completed the trial and could be evaluated, would provide 90% power to detect a mean (±SD) difference of 1.4±7.2 in the average number of migraine days per month. With an anticipated rate of 50%, 130 participants were planned for randomization in this trial. Analyses were conducted in the modified intention- to-treat population, which included all randomly assigned patients who received at least one dose of a trial regimen and had at least 10 days of postbaseline efficacy assessments regarding the primary end point. Safety analyses included all randomly assigned patients who received at least one dose of a trial regimen. Demographic and baseline characteristics were summarized descriptively with a Student’s test for comparison between the two groups and Fisher’s exact test for analysis of contingencies. The primary efficacy outcome was analysed with two-way repeated measure ANOVA followed by the post hoc Bonferroni’s test. The mean change from the baseline with standard errors (±SD) is presented for each treatment group, and the difference versus placebo with 95% confidence interval (CI). For management of missing data in the primary analysis, the average number of headache days per month during the 12-week period was prorated to a 28-day equivalent with the use of all postbaseline observations. The same analyses were used for relevant secondary end points. For the percentage of patients with a reduction of at least 30 to 50% in the average number of headache days per month, the Cochran–Mantel–Haenszel test was used. P<0.05 was considered statistically significant. Adverse events data are collected during the double-blind, placebo-controlled intervention period. The safety population included all the patients who underwent randomization and received at least one dose of a trial regimen. Statistical analysis was performed by Chi-square test for comparison of adverse events between the two groups.
The analyses were carried out with the software GraphPad Prism version 8.4.2, (La Jolla, USA).
Primary end points
After the analysis of their migraine diary, 140 patients were included, for the 28-day observation period. 11 patients were excluded following doctors’ decisions, due to a discrepancy between the results presented in the migraine diary and the data collected after the 28-day observation phase.
A total of 129 patients were randomly assigned to either the Mig-RL group (n = 65) or the placebo group (n = 64). 118 patients received treatments and were included in the study population (Figure 1). A total of 11 patients (9%) across the full duration of the study (Mig-RL, n=6; placebo, n=5) discontinued treatment early. The most frequently reported reasons for early discontinuation were withdrawal by patients (n=4), non-compliance to the protocol (n=3), physician’s decision for suspected pregnancy (n=1), overuse of other medications (n=1), and adverse events (n=1). Overall, 118 of 129 patients (91%) remained in the study until week 12. The demographic data in Table 1 indicated no significant difference between groups.
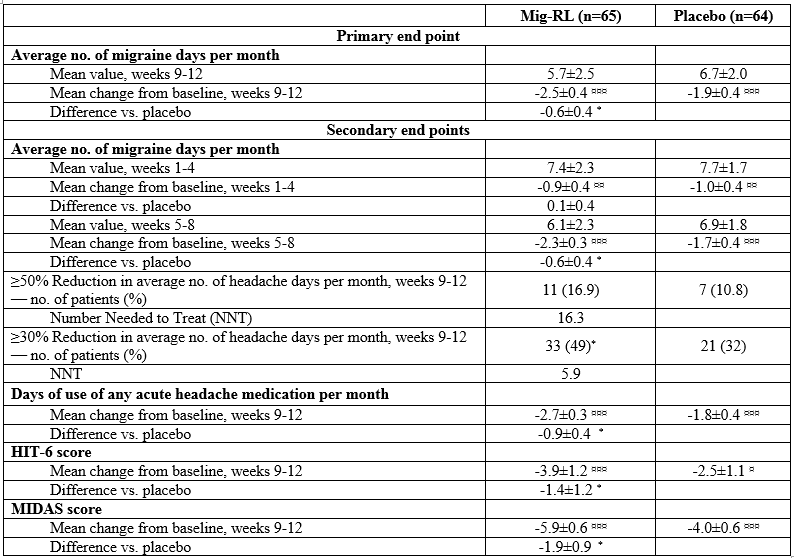
Mig-RL demonstrated statistically significant reduction from the baseline in the frequency of migraine days during weeks 9-12 compared to placebo (-0.6±0.4 [95% confidence interval (CI) -1.26 to -0.09], p=0.01 vs placebo) (Table 2 and Figure 2). Mean of migraine days at baseline (during the 28-day screening period) was 8.4±1.9 in Mig-RL group and 8.7±1.9 in the placebo group. During weeks 9-12, mean of migraine days was 5.7±2.5 and 6.7±2.0 respectively.
Secondary End Points
Weeks 1-4 of treatment did not show any significant difference between the Mig-RL group and the placebo group (Table 2). However, during the weeks 5-8, Mig-RL demonstrated statistically significant reduction from baseline in the frequency of migraine days compared to placebo (-0.6±0.4 [95% confidence interval (CI) -1.20 to -0.04], p=0.02 vs placebo), similarly to weeks 9-12.
The analysis of secondary endpoints showed that 16.9% of patients in the Mig-RL group experienced a reduction of at least 50% in the number of migraine days per month during weeks 9-12, compared to 10.8% in the placebo group (difference from placebo [95%CI] of 5.9% [-5.91% to 17.88%; p=0.06]) with the NNT (numbers need to treat) at 16.71. The ≥30% migraine responder rate for weeks 9-12 was 49% for Mig-RL and 32% for placebo (difference from placebo [95%CI] of 18% [1.22% to 34.69%; p=0.04]) with the NNT at 5.56.
The use of crisis treatments per day was also analysed during the weeks 9-12 and compared to placebo. It revealed a decrease of -2.7 (±0.3) days for the Mig-RL group and -1.8 (±0.4) days for the placebo group, with a difference between both groups of 0.9±0.4 (p=0.03 [95% (CI) -1.20 to -0.04]).

Evolution from baseline in the average number of migraine days per month during the 12-week period after the first dose of the trial regimen in Mig-RL and placebo treated patients. ¥ p<0.05 between Mig-RL and placebo.
HIT-6 scores indicated a decrease of -3.9±1.2 points in the Mig-RL group and -2.5±1.1 points in the placebo group compared to the baseline. The difference between both groups was -1.4±1.2 points (p=0.016 [95% (CI) -5.6 to -0.46]). The MIDAS score followed the same pattern, with a decrease in the Mig-RL group of -5.9±0.6 days versus -4.0±0.6 days in the placebo group, a difference of 1.9±0.9 (p=0.045 [95% (CI) -2.69 to -0.03]).
Safety and adverse events
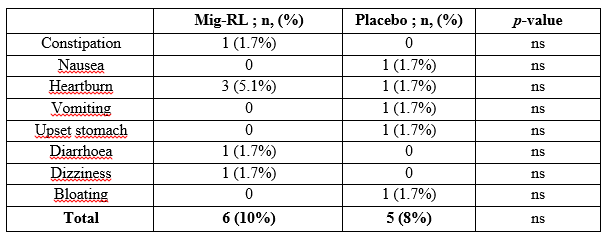
A total of 65 patients received ≥1 dose of Mig-RL and among them 59 patients received the entire treatment (91 doses). 10% of patients in the Mig-RL group experienced either constipation, heartburn, diarrhoea or dizziness (Table 3). Eight percent of patients in the placebo group experienced side effects such as nausea, heartburn, bloating or vomiting. No significant difference was found between the two groups.
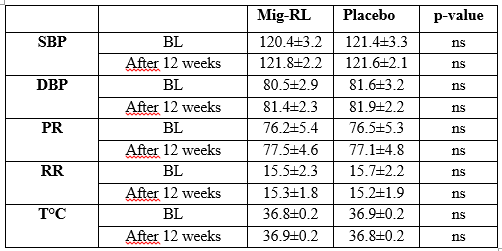
Additional physical examination (Table 4) did not reveal any change of the vital signs or other health parameters in Mig-RL-treated or placebo-treated patients (throughout the trial period or after 12 weeks of treatment).
These results corroborate the observations previously made on an equivalent Mig-RL formulation, where the combination of plants reduced the frequency of migraine attacks by 61.7% over a three-month treatment period in an uncontrolled open study [20]. However, comparison between the present study and the previous one should be limited. First of all, the treatment strategy is different (once a day vs twice a day in the previous trial). Second of all, there is a significant difference in the number of patients (only 14 in the first prospective study, and the absence of a control group, could be a source of bias [20]. Therefore, the present report shows more modest, but more reliable results. However, these results support the conclusions of the meta-analysis of Wider and his colleagues on the efficacy of Tanacetum parthenium in the prophylactic treatment of migraine [14]. Feverfew Mig-99 CO2-extract enriched with parthenolide showed a 2.8-day reduction in migraine days per month in the treated group of a randomized, double-blind, placebo-controlled study [25]. Mig-RL treatment also has a high parthenolide content (0.75 mg per day) and its presence may explain its beneficial role in preventing migraine attacks. In fact, studies that do not show the efficacy of Tanacetum parthenium rarely have a dosed parthenolide level. However, it is now well established that the biological properties of feverfew are mainly due to the presence of parthenolide [11]. The extraction methods but also the sourcing of the plant (origin, harvest date, storage condition) and the parts used, are important conditions for optimizing the concentration of parthenolides in the extract [12].
Propranolol is the most common preventive treatment for migraines [26]. Studies have shown that it effectively reduces the number of attacks per month by 1.3 (-2.0 to -0.62) days after 12 weeks of treatment [27]. Topiramate, another common preventive treatment, reduces the amount of migraine days per month by 0.9 (-1.3 to -0.39) [27]. However, like most preventive treatments, topiramate is also not a migraine-specific treatment. Large daily doses of these non-specific treatments can cause many adverse effects [28]. Today, some patients prefer natural treatment rather than synthetic drugs and Tanacetum parthenium enriched with parthenolide may be a help for these patients. Results of this study show that associating Tanacetum parthenium and Salix Alba is slightly effective compared to similar treatment but may represent a natural and safe additional help [27].
The mechanism of action of Tanacetum parthenium in migraine prophylaxis is potentially related to the antispasmodic activity on smooth muscle vessels [29] and the anti-serotoninergic effect of parthenolide on blood platelets [13], [30]. It also has anti-inflammatory properties, resulting mainly from the inhibition of pro-inflammatory cytokines and interleukins. This inhibitory activity could be due to an action on the NF-κB pathway [31]. Another more recent theory suggests that parthenolide desensitizes the TRPA1 receptor in nociceptive neurons of the trigeminovascular system [32]. Therefore, evaluating the role of Tanacetum parthenium alone or in association with Salix alba on TRPA1 receptor desensitization, could provide a better understanding of the mode of action of Mig-RL.
The present investigation shows that the combination of these two plants, probably with additive or synergistic pharmacological properties, can act together to prevent migraine attacks. The migraine prophylaxis properties of Salix alba were never clinically evaluated as all the studies were directed to study analgaesic properties of its active ingredient, the salicylic acid or aspirin [33]. Salicylate derivatives, particularly salicin, have anti-inflammatory properties in Salix alba and its efficacy has been demonstrated for chronic joint and muscle pain [34]. Its efficacy is believed to be caused by the inhibition of pro-inflammatory cytokines, TNF-α, COX-2 and an action on the NF-κB pathway [35]. Other authors have also demonstrated the modulating effect of salicin on serotonin [36]. In the management of migraines, aspirin has only been evaluated as a crisis treatment because of its important digestive side effects [37]. It has never been proven to be effective as a prophylactic treatment [38]. The anti-inflammatory properties of Salix alba and its probable serotonin-modulating capacities may contribute synergistically to enhancing migraine prophylaxis properties of Tanacetum parthenium [39]. Whether higher migraine preventive properties of the association of plants compared to Tanacetum parthenium alone are due to additive or synergistic, analgaesic or anti-inflammatory action of Salix alba, is not clear and require further investigation.
Tanacetum parthenium combined with Salix alba were tested in an in vitro mouse model of migraine showed invasive cortical depression [17], a phenomenon potentially implicated in the appearance of migraine auras [40]. Results show a greater decrease in oxidative stress, inflammation and serotonin release when these plants are combined.
Only a few isolated and minor side effects were reported and overall Mig-RL was well tolerated by patients. Five percent of patients experienced heartburn-type side effects which may be due to the presence of salicin. The safety profile of Tanacetum parthenium is also corroborated by its use in the paediatric population (at a dose higher than in the present study) without any severe side effect [41]. In recent years, new specific treatments have been developed, such as monoclonal antibodies which target the CGRP or its receptor [42], representing a major advance in migraine prophylaxis but the cost of these treatments may limit its widespread use. This clinical trial shows that Mig-RL, a combination of Tanacetum parthenium and Salix alba, could provide a safe additional help to the prophylactic treatment of migraine attacks.
We acknowledge that a major limitation of this study is the large number of patients lost even before the randomization process, thus reducing the groups to a statistically acceptable minimum. The absence of other clinical studies for this association of plants in the treatment of migraine also limits the interpretation of the results. These are a first orientation which opens new perspectives in the prophylactic treatments of migraine.
We have shown the therapeutic effect of an association of Tanacetum parthenium with willow bark. The main active ingredients, parthenolide and salicin respectively, are the key components that may explain this effect in the prevention of migraines [39]. Unfortunately, the oral administration results in a higher degradation of the active ingredients through the digestive system. We are currently working on the development of a nasal spray form of injection to avoid a too important degradation of the active ingredients.
The design and conduct of the trial and data analysis were supported by a grant from VITROBIO & NATURVEDA SAS (ZAC de Lavaur 63500 ISSOIRE, France), the manufacturer of Mig-RL. We thanks the patients who participated in this trial and their families; all investigators, site personnel and coordinating investigators. We also strongly thanks Dr. Xavier MOISSET (CHU Clermont-Ferrand, France) for his precious help in writing the article and Dr. GREMEAU-RICHARD Christelle (Neuro-dol INSERM 1107, France) for her corrections to the protocol.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
